Targeted Therapy vs Chemotherapy vs Immunotherapy, Explained Clearly
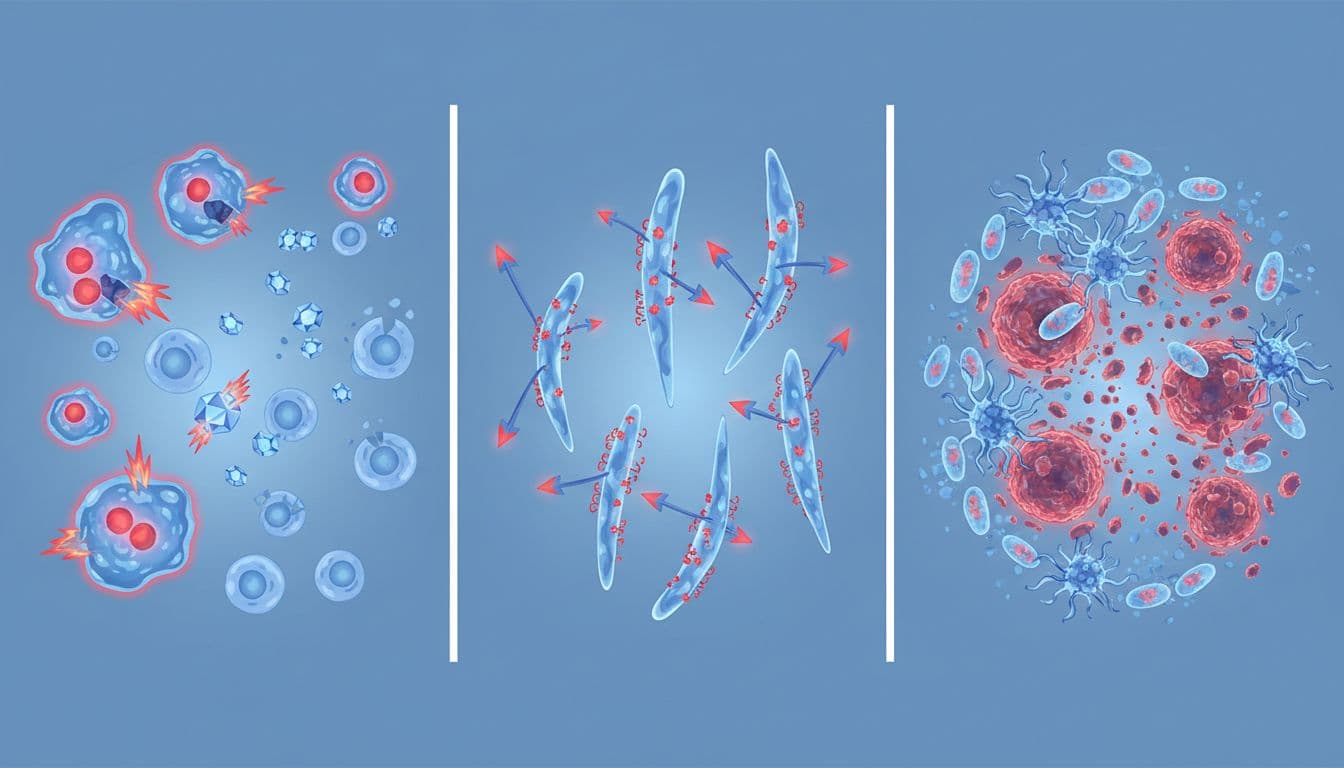
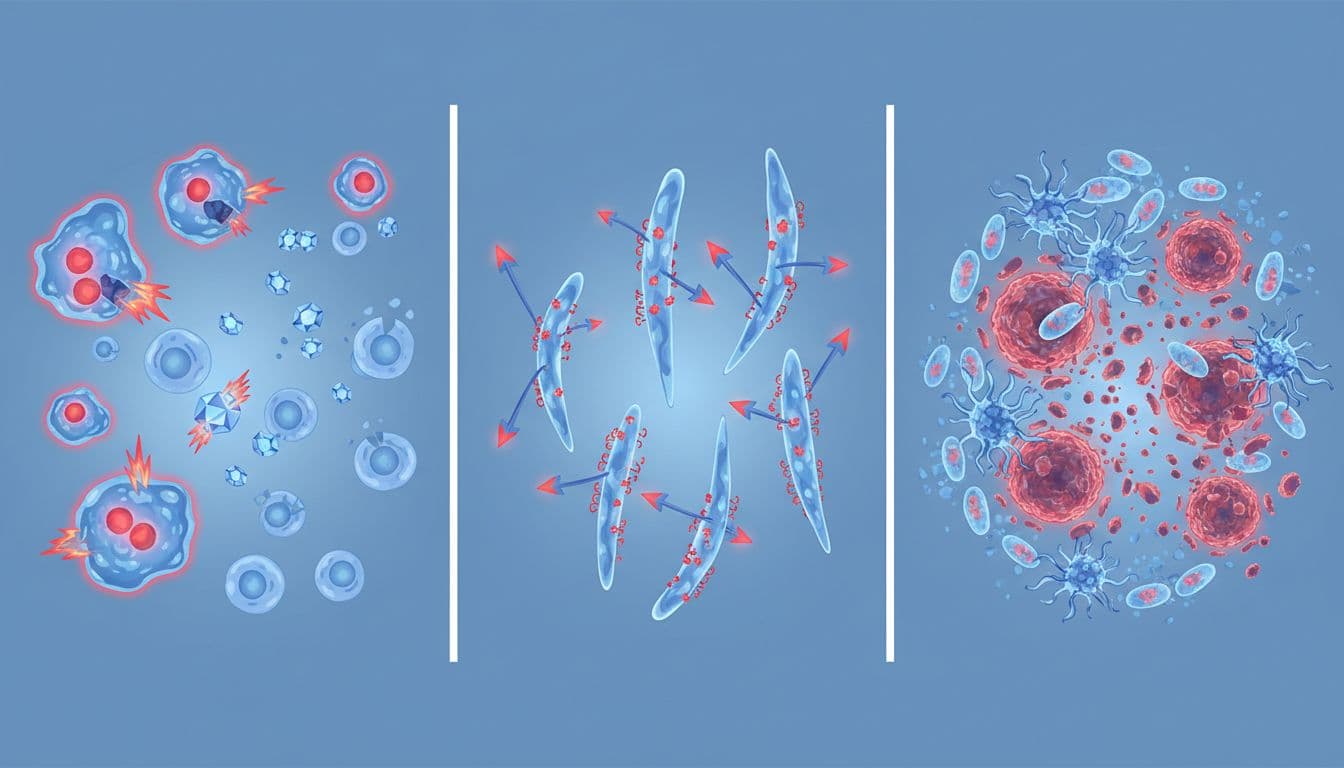
Trying to compare targeted therapy vs chemotherapy vs immunotherapy can feel like sorting through three tools that all fight cancer in different ways. The short answer is simple, chemotherapy attacks fast-growing cells, targeted therapy blocks specific cancer signals, and immunotherapy helps the immune system find and fight cancer.
Short answer: None is automatically the "best" treatment. The right choice depends on the cancer type, stage, biomarker results, your overall health, and the goal of care. In many cases, doctors also combine these treatments.
If you're a patient or caregiver, that difference matters because each option can bring a different chance of response, side effect pattern, cost, and treatment schedule. This information is for educational purposes only, and treatment choices should always be reviewed with a licensed oncology team.
How each cancer treatment works inside the body
Chemotherapy is the oldest of the three approaches, but it still matters. Think of it like a weed killer that hits anything growing fast. Cancer cells often grow quickly, so chemo can shrink tumors or slow spread. However, hair follicles, the gut lining, and bone marrow also grow fast, so they can get caught in the crossfire.
Chemotherapy attacks fast-growing cells, both cancer and some healthy cells
That broad action explains common side effects such as hair loss, nausea, fatigue, low blood counts, and higher infection risk. Even so, chemotherapy remains a standard treatment for many cancers. Doctors may use it before surgery to shrink a tumor, after surgery to lower the risk of return, or in advanced disease to control cancer quickly.
Targeted therapy blocks the signals cancer cells need to grow
Targeted therapy works more like a lock-and-key system. It looks for a specific weakness, such as a gene mutation or an overactive protein. If that target is present, the drug can interfere with the signal that tells cancer cells to grow or survive.
For example, trastuzumab targets HER2-positive breast cancer. In prostate cancer, Xtandi (Enzalutamide) 40mg soft capsules block androgen signaling, which is one reason Enzalutamide is often described as a hormone-signaling targeted treatment. Other targeted drugs, such as Tagrisso (osimertinib) for EGFR-mutated lung cancer, only make sense when testing shows the right mutation. That is why SITC consensus guidance on essential biomarkers and routine tumor testing play such a large role in modern cancer care.
Immunotherapy helps the immune system recognize and fight cancer
Immunotherapy does not directly poison cancer cells the way chemotherapy does. Instead, many drugs remove immune "brakes," especially checkpoint inhibitors that target PD-1, PD-L1, or CTLA-4. Once that brake comes off, immune cells may attack the tumor more effectively.
A special form, CAR T-cell therapy, uses lab-engineered immune cells and is used mainly in some blood cancers. Side effects differ from classic chemo. Rather than hair loss or severe nausea alone, immune-related problems can affect the lungs, colon, liver, skin, or hormone glands because the immune system may also attack healthy tissue.
The biggest differences in benefits, limits, and side effects
Most people want to know which option is more precise, which works fastest, and which causes fewer whole-body side effects. The answer depends on the cancer's biology, not only the drug category.
This quick comparison helps set expectations:
| Treatment | Main strength | Main limit | Common side effect pattern | | | --- | --- | --- | | Chemotherapy | Broad reach, often acts fast | Less selective | Hair loss, nausea, fatigue, low counts | | Targeted therapy | More precise when marker is present | Won't work without the target | Rash, diarrhea, liver or heart effects, varies by drug | | Immunotherapy | Can create long responses in some cancers | Not all tumors respond | Immune-related inflammation, fatigue, skin and gut issues |
The main takeaway is that precision often comes with a condition. Targeted therapy needs the right target. Immunotherapy needs the right immune setting. Chemotherapy can still work when neither of those is present. Recent overviews, including this comparison of targeted therapy and immunotherapy in oncology, note that newer treatments may improve survival and quality of life in selected patients, but they do not replace chemo in every case.
When chemotherapy may still be the best fit
Chemotherapy can work across many cancer types. It may shrink tumors quickly, which matters when symptoms are urgent or the cancer is widespread. It also remains useful when no known mutation or protein target is found. Its broad reach is both its strength and its weakness.
When targeted therapy or immunotherapy may offer an advantage
When a tumor carries the right marker, targeted therapy can be more focused. HER2-positive breast cancer, EGFR-mutated lung cancer, and some BRCA-related cancers are common examples. Immunotherapy can sometimes produce long-lasting control, especially in melanoma, lung cancer, kidney cancer, and some blood cancers. In metastatic melanoma, long-term survival improved sharply after checkpoint inhibitors entered routine care.

Who may be a good candidate for each treatment option
Doctors rarely choose treatment based on one factor. They look at cancer type, stage, prior treatments, age, organ function, other health conditions, and what matters most to the patient. A drug that looks strong on paper may still be the wrong fit if the side effects clash with daily life or other illnesses.
Why biomarker testing matters before treatment starts
Biomarker testing helps match the right medicine to the right patient. Targeted therapy usually requires a confirmed target. Some immunotherapy decisions also depend on markers such as PD-L1, MSI-H, or tumor mutation burden. A recent review of predictive biomarkers in cancer immunotherapy shows how much treatment planning now depends on these results.
Why side effect history and daily life also shape the plan
Daily routine matters more than many people expect. Some treatments are pills taken at home. Others require infusions every few weeks. A person who lives far from a cancer center may prefer an oral targeted drug when it is clinically appropriate. Another patient with autoimmune disease may not be a good immunotherapy candidate because the immune system is already overactive.
Combination treatment is also common now. Chemo plus immunotherapy is routine in several cancers, and targeted therapy may come before or after other treatments. For example, a patient with advanced lung cancer and a strong EGFR mutation profile may start with a pill rather than infusion-based chemotherapy. In contrast, a patient with fast-growing cancer and no actionable marker may still begin with chemo.

Cost, access, and safe ways to get cancer medicines
Cost can shape real-world treatment as much as biology does. In the USA, many newer targeted therapy and immunotherapy drugs carry very high prices. Chemotherapy costs vary more widely because some older agents are generic, while supportive care, infusion center charges, and monitoring still add up. Prices can also differ in the UK and Australia because of different health systems and pricing rules.
For oral cancer medicines, some patients compare options through an Online Pharmacy. That can be reasonable, but only if it is a legitimate online mail order pharmacy that requires a valid prescription, follows licensed pharmacy standards, and verifies the order before shipping. If you're comparing sources, guides on generic vs brand-name cancer medicines can help frame the discussion.
How patients can compare affordability without risking safety
Check a few basics before ordering:
- The pharmacy asks for a valid prescription and pharmacist review.
- The listing clearly states the brand or generic version.
- Shipping timelines are realistic, with tracking when available.
- The medicine is appropriate for home delivery, because some drugs must be given in a clinic.
This matters because many cancer medicines are costly. People often compare prices for Enzalutamide, and public price trackers such as Enzalutamide prices and discounts show how wide the price gap can be. Some targeted medicines, such as oral palbociclib for HR-positive breast cancer, are taken at home, while others, such as nivolumab injection immunotherapy, still require clinic-based infusion planning.
Examples of high-cost medicines patients often research
Enzalutamide is one example because long treatment periods can make cost a major issue. Some people also search for Upadacitanib through an Online Pharmacy, usually meaning upadacitinib. That drug is not a cancer treatment and sits outside the three cancer treatment types covered here. If that search comes up in your household, this upadacitinib FAQ guide may help separate it from oncology care.

Common questions patients ask about targeted therapy, chemotherapy, and immunotherapy
Is targeted therapy safer than chemotherapy?
Often, but not always. Targeted therapy usually affects fewer healthy cells, so it may cause fewer whole-body side effects. Still, it can trigger serious problems such as liver injury, heart effects, lung inflammation, or high blood pressure, depending on the drug.
Is immunotherapy better than chemotherapy?
Not across the board. Immunotherapy can produce longer responses in some cancers, especially when the tumor is a good match. Yet many patients still need chemotherapy first, or receive both together, because immunotherapy alone does not work for every cancer type.
Can you take chemotherapy and immunotherapy together?
Yes. Combination treatment is common in lung cancer and several other cancers. The goal is often to get the faster tumor control of chemotherapy plus the longer immune response that immunotherapy may provide. Your doctor chooses this based on evidence for your exact cancer.
How do doctors know if targeted therapy will work?
They use biomarker testing. That may include tumor tissue testing, blood-based testing, or both. If the tumor lacks the needed mutation or protein target, the drug is unlikely to help, even if it works well in other patients.
Which treatment usually causes the most side effects?
Chemotherapy tends to cause the most classic whole-body side effects because it affects many fast-growing cells. Immunotherapy side effects can be less frequent but sometimes more unpredictable. Targeted therapy often falls in between, with side effects linked to the exact pathway being blocked.
Conclusion
The best way to think about these three treatments is simple. Chemotherapy is broad, targeted therapy is selective, and immunotherapy recruits your immune system. Fit matters more than hype.
If you or a loved one is comparing cancer medicines, focus on the diagnosis, biomarker results, side effect history, and safe access. Then review affordability and refill options only through licensed sources that verify prescriptions and support follow-up care.