Top 10 Most Expensive Drugs in the U.S. (2026 Medicare Spending Report)

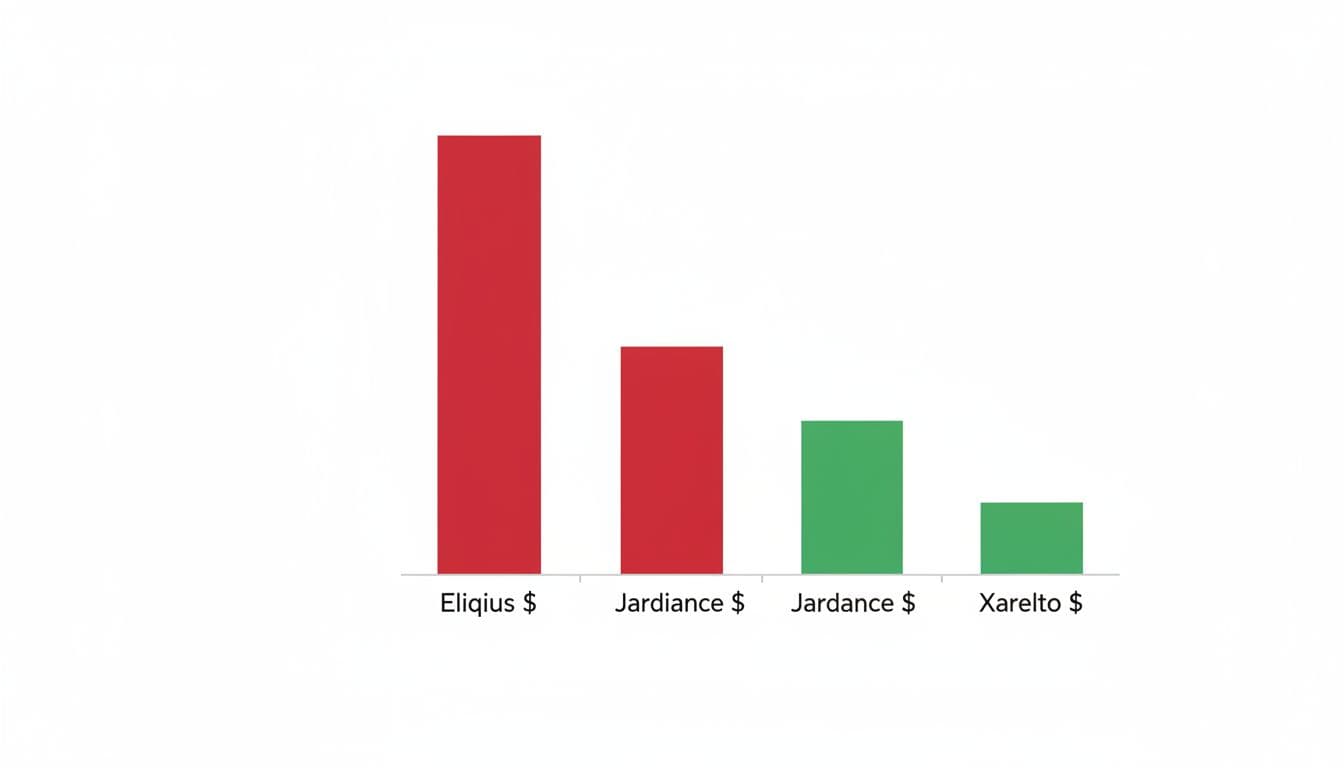
In 2026, a small group of prescription drugs is driving a huge share of Medicare spending, with Eliquis alone reaching about $20.8 billion and other top drugs, like Jardiance, Xarelto, and Keytruda, adding billions more. In this report, "most expensive" means the highest total spending across Medicare, not the highest price per pill, dose, or single prescription.
That distinction matters if you're trying to understand why blood thinners, diabetes drugs, autoimmune treatments, and cancer medicines keep pushing system-wide costs higher, even when patients pay very different amounts out of pocket. If you're also trying to buy cancer medication in generic alternative form, it helps to understand the gap between brand pricing, patient costs, and total spending, plus how generic vs brand cancer medicines and why cancer drugs are pricey in the US shape what you see at the pharmacy counter.
Next, let's look at the 10 drugs that account for the biggest share of Medicare drug spending.
The 10 drugs that drove the biggest prescription spending in 2026
This list is about total spending, not sticker shock alone. In other words, the drugs that drain the most dollars are often the ones used month after month by huge numbers of people, plus a few specialty medicines that carry very high per-patient costs.
CMS price negotiation starts to change what Medicare pays in 2026, but these medicines still sit near the top because demand remains strong and treatment often lasts for years. You can also see how those negotiated prices fit into the broader policy picture in CMS's selected drugs and negotiated prices list.

Quick profile of each drug, what it treats, who makes it, and where the money goes
A fast scan helps show why these names keep surfacing in Medicare spending data. Some win on sheer volume, while others stay high because each patient needs a costly specialty therapy.
- Eliquis (Bristol Myers Squibb, Pfizer)
Treats atrial fibrillation and blood clots. Demand stays high because stroke prevention is long-term and common in older adults.
Most of the cost burden comes from chronic daily use across a very large patient base. - Jardiance (Boehringer Ingelheim, Eli Lilly)
Used for type 2 diabetes, heart failure, and chronic kidney disease. Its reach expanded because one drug now serves several common conditions.
Spending rises from broad uptake and repeat fills, not from a one-time ultra-high price. - Xarelto (Janssen)
Another major blood thinner for clot prevention and stroke risk reduction. It serves many of the same high-need patients as Eliquis.
Here, the pressure comes from long-term treatment and limited low-cost brand competition for years. - Farxiga (AstraZeneca)
Treats type 2 diabetes, heart failure, and kidney disease. It became a go-to drug because doctors use it across several chronic illnesses.
The dollars pile up through high-volume use in conditions that rarely end after a short course. - Januvia (Merck)
A diabetes drug with years of wide prescribing, especially among older adults. It remains familiar, easy to continue, and often stays on regimens for long periods.
Its spending story is mostly about maintenance therapy, not specialty status. - Entresto (Novartis)
Used in heart failure, where patients often need ongoing therapy to stay stable and avoid hospitalization.
The spending burden comes from lifelong treatment patterns in a large, medically complex population. - Stelara (Johnson & Johnson)
Treats psoriasis, psoriatic arthritis, Crohn's disease, and ulcerative colitis. Fewer patients use it than Eliquis, but each treatment course is expensive.
This is a classic specialty drug case, with high per-patient cost and historically limited direct competition. - Enbrel (Amgen)
Prescribed for rheumatoid arthritis and other inflammatory conditions. Many patients stay on it for years because these diseases flare when treatment stops.
Spending remains high due to biologic specialty pricing and chronic use. - Fiasp/NovoLog insulin products (Novo Nordisk)
These insulins treat diabetes, a condition that doesn't take a month off. Even when policy caps help patients, national spending stays large because so many people need insulin.
The cost burden comes from constant refill demand and the sheer size of the diabetes population. - Imbruvica (AbbVie, Johnson & Johnson)
Treats blood cancers such as CLL and mantle cell lymphoma. Patient volume is much lower than for diabetes or heart drugs, but each course can be very expensive.
Its ranking comes mainly from specialty oncology pricing and long treatment duration, which is why people trying to buy cancer medication in generic alternative form often start by comparing options like generic Ibrutinib for CLL.
For cancer patients, this is where the spending story gets more personal. A national top-10 list may track Medicare's burden, but families often feel the pressure one refill at a time. If you're comparing treatment types, this guide on immunotherapy and targeted cancer drugs explained can help frame why some oncology medicines cost so much and why access paths differ.
Why this list is filled with chronic disease drugs, not just rare disease therapies
At first glance, you might expect the list to be packed with rare disease drugs or gene therapies. Some of those products have far higher one-time prices. But this ranking tracks total national spending, and that's a very different contest.
Think of it like rain versus a burst pipe. A burst pipe is dramatic and expensive in one moment. Rain, though, can fill the whole reservoir if it falls every day. That's what drugs like Eliquis, Jardiance, Xarelto, and Farxiga do. They serve huge populations, often for years, so total spending keeps compounding.

A rare therapy may cost more per patient than anything on this list. Lenmeldy is a useful contrast because it shows how a treatment can have a stunning price tag yet still not dominate national spending if only a tiny number of patients receive it. By contrast, KFF's Medicare drug negotiation overview highlights how a small group of heavily used drugs accounts for an outsized share of Part D costs.
The big driver is not always the highest price per dose. Often, it's the combination of high use, long duration, and common chronic disease.
That's also why the top 10 isn't just a cancer list. Cancer drugs like Imbruvica are expensive, but millions of patients do not take them. Blood thinners, diabetes pills, heart failure drugs, and insulin do something more powerful from a budget standpoint, they show up every month, in huge numbers, across the country.
For readers focused on oncology costs, that distinction matters. A medicine can be financially crushing for one household and still rank below a common chronic drug in total Medicare spend. If you're comparing targeted cancer treatment costs, options like generic Olaparib for BRCA cancers or generic Enzalutamide for prostate cancer show why many patients look beyond the brand name when they need long-term therapy.
What makes these drugs so expensive in the first place
High Medicare spending does not happen by accident. In most cases, it comes from a mix of protected pricing power, slow competition, and the high cost of making and delivering advanced treatments. That is why drugs like Stelara, Enbrel, and Imbruvica can stay near the top of spending lists even when the number of patients taking them is far smaller than for common diabetes or heart medicines.
Price also reflects timing. Some drugs reached the market years ago and still faced limited pressure from cheaper rivals, while others belong to complex categories where follow-on versions take longer to launch. As KFF's overview of Medicare drug negotiation points out, many of the drugs targeted for negotiation were high-spend products with little or no generic or biosimilar competition.
Patent protection and weak generic competition keep brand prices high
One of the biggest reasons drugs stay expensive is simple, competition arrives late. A brand drug with patent protection, or related exclusivity protections, can keep prices elevated because no true low-cost rival is allowed to enter right away. That matters even more when the drug treats a serious illness and doctors are reluctant to switch stable patients unless a clearly approved alternative is available.

In cancer care, that delay hits hard. Many patients try to buy cancer medication in generic alternative form when it becomes available, because the savings can be dramatic. Yet for newer oncology drugs, especially targeted therapies and infused treatments, those options are often thin or delayed. Imbruvica is a good example. It has been a major blood cancer drug, but lower-cost competition has not reshaped the market the way patients might expect. For readers comparing options, affordable generic equivalent to Imbruvica shows how important a generic path can be when it exists.
The same pattern shows up with biologics. These drugs do not get traditional generics. They get biosimilars, which are harder and slower to bring to market. As a result, a drug can sit in a kind of pricing moat for years. Reports tracking IRA negotiations have highlighted Stelara and Enbrel as major examples of high-spend drugs where biosimilar competition has been limited or delayed, including coverage from Center for Biosimilars on new CMS prices and biosimilar market analysis for Enbrel and Stelara.
Think of it like a toll road with very few exits. If patients and health plans have only one reliable route, the owner of that road can keep charging premium rates. Until real competition arrives, brand prices usually stay sticky.
When a drug has little direct competition, the list price often reflects market power as much as medicine.
Biologics, cancer drugs, and specialty medicines cost more to make and manage
Some drugs are expensive because they are protected. Others are expensive because the whole system around them costs more. Stelara, Enbrel, and Imbruvica all sit in a specialty-drug tier, where manufacturing, storage, handling, and patient monitoring are more demanding than they are for standard pills.

Stelara and Enbrel are biologics, which means they are produced through living systems, not mixed like a simple tablet. That usually requires tightly controlled manufacturing, cold-chain shipping, and more testing along the way. A small problem in production can ruin a batch, so the margin for error is low. If you look at a product like Stelara Ustekinumab 90mg injection, you are not just paying for a dose. You are paying for a complex chain of production and delivery that starts long before the medication reaches a patient.
Cancer drugs add another layer. Imbruvica is an oral targeted therapy, which sounds simpler than an infused oncology drug, but it still comes with high development costs, careful monitoring, and use in a narrower patient group. Unlike a common blood pressure drug, a cancer medicine may serve a much smaller population. That means companies spread research, approval, and support costs across fewer patients, which can keep per-patient prices high. For Medicare, even a smaller user base can still drive billions in spending when treatment lasts for months or years. Coverage of Imbruvica's negotiated Medicare price change reflects how large those costs became before negotiated discounts began.
Specialty drugs also tend to bring extra care steps that patients do not always see on the bill:
- They may need special shipping and storage, especially if refrigeration is required.
- They often require prior authorization and ongoing monitoring, which adds administrative cost.
- They may involve nurse training, infusion services, or side-effect management, depending on the drug.
- They usually treat serious, long-term conditions, so patients stay on therapy longer.
That is why these medicines do not behave like ordinary retail prescriptions. A low-cost generic tablet can move through the system like a commuter car. A specialty biologic moves more like a refrigerated cargo plane, slower, costlier, and harder to replace. And when that medicine treats cancer or severe autoimmune disease, demand stays strong even at a very high price.
How 2026 policy changes could lower costs for patients
The biggest policy shift in this report is simple: some of Medicare's highest-spend drugs now have negotiated prices in 2026. That won't erase high drug costs across the whole U.S. market, but it does change the math for many people in Medicare Part D.
For readers scanning headlines, here's the plain-English version. Medicare negotiation can lower what Medicare pays for certain drugs, and that can reduce out-of-pocket costs for eligible Part D enrollees. Still, the savings are not one-size-fits-all, and they do not automatically flow to people with employer plans or commercial insurance.
Which top-spend drugs are getting negotiated Medicare prices
The first negotiated-price group lines up closely with this top-spend list. The drugs in this report that are part of the first 2026 Medicare negotiation group are:
| Drug | Main use area | In the first negotiated-price group for 2026? |
|---|---|---|
| Eliquis | Blood thinner | Yes |
| Jardiance | Diabetes, heart failure, kidney disease | Yes |
| Xarelto | Blood thinner | Yes |
| Januvia | Type 2 diabetes | Yes |
| Farxiga | Diabetes, heart failure, kidney disease | Yes |
| Entresto | Heart failure | Yes |
| Enbrel | Autoimmune disease | Yes |
| Imbruvica | Blood cancer | Yes |
| Stelara | Autoimmune disease | Yes |
| NovoLog / Fiasp | Insulin | Yes |
That matters because these are not fringe products. They are widely used, long-term therapies, or costly specialty medicines that have put heavy pressure on Medicare spending for years. According to KFF's Medicare drug negotiation overview, the first round focused on high-spend Part D drugs with limited low-cost competition. Real-time 2026 updates also show negotiated prices ranging from major cuts to very steep ones, with some products dropping by well over half from prior pricing benchmarks.
In practical terms, these changes mainly affect Medicare Part D, not every insurance card in America. If you're enrolled in a Part D plan and take one of these drugs, your share of the cost may fall depending on your plan design, deductible status, and where you are in the benefit year. That's why one patient might feel the savings right away, while another notices them more gradually over time.

For a drug like generic Eliquis Apixaban, the policy story is especially visible because it has been one of Medicare's biggest spending drivers. The same goes for heart failure treatment, where generic Entresto Sacubitril/Valsartan sits at the center of a large and medically complex patient population. When Medicare pays less for drugs like these, many eligible beneficiaries can pay less too, although the exact amount still depends on plan rules.
The key point is not that every patient gets the same discount. It's that Medicare Part D now has a lower negotiated ceiling on some of its most expensive drugs.
This also matters for cancer patients. Imbruvica is on the negotiated list, which may help some Medicare users, but people trying to buy cancer medication in generic alternative form should know that negotiation and generic competition are two different things. One lowers Medicare's negotiated payment for a selected brand drug. The other can reshape the whole market when approved alternatives become available.
What these price cuts do, and do not, change for people with private insurance
Here's where many headlines get fuzzy. Medicare negotiation does not set a national price for everyone. It creates a negotiated price within Medicare for selected drugs, mainly through Part D. If you have employer coverage, an ACA marketplace plan, or another private policy, your insurer still uses its own contracts, formularies, and cost-sharing rules.
Think of Medicare negotiation like lowering the fare on one major train line. It's a big deal for people on that line. But it doesn't mean every bus, flight, and toll road suddenly gets cheaper too. Private plans still run on a different map.
Several factors can still decide what you pay with private insurance:
- Your deductible may force you to pay a large upfront share before coverage really kicks in.
- Your copay or coinsurance may be tied to a specialty tier, not the headline drug price.
- Your plan's formulary may prefer one drug over another, even within the same treatment class.
- Prior authorization can delay access or require proof that cheaper options failed first.
- Some plans use copay accumulator or specialty pharmacy rules that change how savings programs help.
That is why two people taking the same medicine can face very different bills. One may pay a flat copay. Another may owe a percentage of the drug's cost. A third may need approval before the first fill. The medicine is the same, but the benefit design acts like a different set of rules at the register.
For example, Medicare's negotiated price for Imbruvica may help a qualifying Part D patient, but a privately insured cancer patient might still face a high coinsurance bill, specialty pharmacy requirements, or utilization review. The same logic applies to Enbrel, Stelara, and other specialty drugs. As AARP's summary of the first Medicare-negotiated drug prices explains, the 2026 savings are targeted to Medicare beneficiaries, not the entire commercial insurance market.
This is also why price headlines can feel frustrating. You read that a drug price was cut, then your next refill looks almost the same. In many cases, the headline is true, but it applies to a different payer, a different coverage channel, or a different phase of the benefit.
If you have private insurance, the useful takeaway is this: don't assume a federal price announcement will match your pharmacy bill. Check your plan's formulary, look at your deductible, and confirm whether prior authorization applies. And if you're comparing expensive therapies, including options to buy cancer medication in generic alternative form where available, focus on your actual benefit design, not just the national headline.
How patients can compare costs, ask about lower-price options, and plan ahead
High drug spending makes headlines, but your own bill still comes down to the details, your plan, your refill timing, and whether a lower-cost option exists. A little homework can shave off real dollars without changing the quality of care. That's especially true for people trying to buy cancer medication in generic alternative form, where the safest savings come from verified products, matched dosing, and prescriber oversight.
Smart ways to lower your prescription bill without risking your care
Start with the simplest question: Is there a generic? If not, ask whether a biosimilar is available for a biologic drug. Generics use the same active ingredient as the brand, while biosimilars are highly similar versions of complex biologic medicines. Either can move a prescription to a lower formulary tier and cut what you pay.

It also helps to compare the covered alternatives in your plan. Two drugs may treat the same condition, yet one lands on a cheaper tier. If you're on Medicare, 2026 rules matter here because Part D now caps annual out-of-pocket drug costs, and negotiated prices affect some top-spend drugs, as outlined in KFF's Medicare drug negotiation overview.
A few practical moves often make the biggest difference:
- Ask your prescriber to review generic availability and any therapeutic alternatives your plan prefers.
- Check whether a 90-day supply makes sense for a stable, long-term medicine. It can lower per-fill costs and reduce missed refills.
- Review your plan's mail-order or refill tools if you use ongoing treatment, including home delivery of expensive generics.
- Watch refill timing if you have Medicare or a high deductible plan. Your monthly explanation of benefits can show where you are in coverage, which helps you avoid surprises and plan before any gap or reset hits.
- If you take specialty oncology drugs, compare exact products and strengths, such as generic Xtandi enzalutamide 40mg, only after your clinician confirms it fits your treatment plan.
The safest way to save is to compare equivalent treatment options, not to improvise your own switch.
For people with Medicare, Part D cost-saving options can also help if monthly costs still feel heavy.
Do's and don'ts before switching from a brand-name drug to a lower-cost option
A lower price is good news, but only if the medication still matches your care plan. Think of a switch like changing tires on a moving car, it can be done well, but only with the right fit.
Do:
- Talk to a licensed prescriber or pharmacist before making any change.
- Confirm the exact active ingredient, strength, and dosage form match what was prescribed.
- Check your insurer's formulary and copay so the "cheaper" option is actually cheaper.
- Ask whether the lower-cost option needs new monitoring, prior authorization, or a new prescription.
- Use verified pharmacies and trusted sources when comparing options, especially for specialty drugs like Tagrisso osimertinib for NSCLC.
Don't:
- Don't stop treatment or switch products on your own because of price alone.
- Don't split specialty tablets, capsules, or oncology drugs unless your clinician says it's safe.
- Don't assume two similar brand names are interchangeable.
- Don't buy from unverified sellers offering steep discounts with no prescription checks.
- Don't ignore refill timing, because running out can cost more than the drug itself if it interrupts treatment.
Conclusion
The clearest takeaway from this 2026 data report is that the biggest drug costs in the U.S. come from two forces working together, huge patient demand and too little lower-cost competition. That's why common long-term therapies and a few high-price specialty drugs continue to dominate spending, even as negotiated Medicare prices begin to trim some of the damage.
Still, 2026 is a starting point, not a fix. Affordability pressure remains high, especially for patients who need ongoing treatment or want to buy cancer medication in generic alternative form, whether that means comparing options like generic Cyclophosphamide for cancer treatment or tracking when broader competition finally reaches the market.
Watch what happens next with generic launches, biosimilar uptake, and future Medicare negotiation rounds. Those three shifts will do more than any headline to decide who actually pays less at the pharmacy counter.